

Treating aortic stenosis is no longer simply about replacing a diseased heart valve—it is about preparing patients for the years and decades that follow, according to structural heart disease expert Dr. Guilherme Silva during the Rodolfo Soto Memorial Lecture at the 56th Philippine Heart Association-Philippine College of Cardiology (PHA-PCC) Annual Convention and Scientific Meeting.
In his lecture, “Lifetime Management of Aortic Stenosis: Are We in the Business of Predicting the Future?”, Silva challenged clinicians to think beyond the immediate success of a procedure and instead consider how today’s decisions may affect a patient’s future treatment options.
Aortic stenosis, the most common type of heart valve narrowing, restricts blood flow from the heart to the rest of the body. As the condition progresses, the heart must work harder to pump blood, eventually leading to symptoms such as chest pain, shortness of breath, and fainting.
While advances in treatment have dramatically improved outcomes, Silva emphasized that physicians must now consider a broader question: what happens when the replacement valve eventually wears out?
“We are not necessarily in the business of predicting the future,” Silva said. “We are in the business of preparing patients for it.”
Silva reflected on the early years of transcatheter aortic valve replacement (TAVR), when the procedure was reserved primarily for patients considered too sick or too high-risk for surgery.
He recalled treating a critically ill woman who arrived in cardiogenic shock after previous aortic surgery and severe valve disease.
With surgery considered too risky, the team stabilized her using mechanical circulatory support before proceeding with a transcatheter valve implantation under extremely challenging conditions.
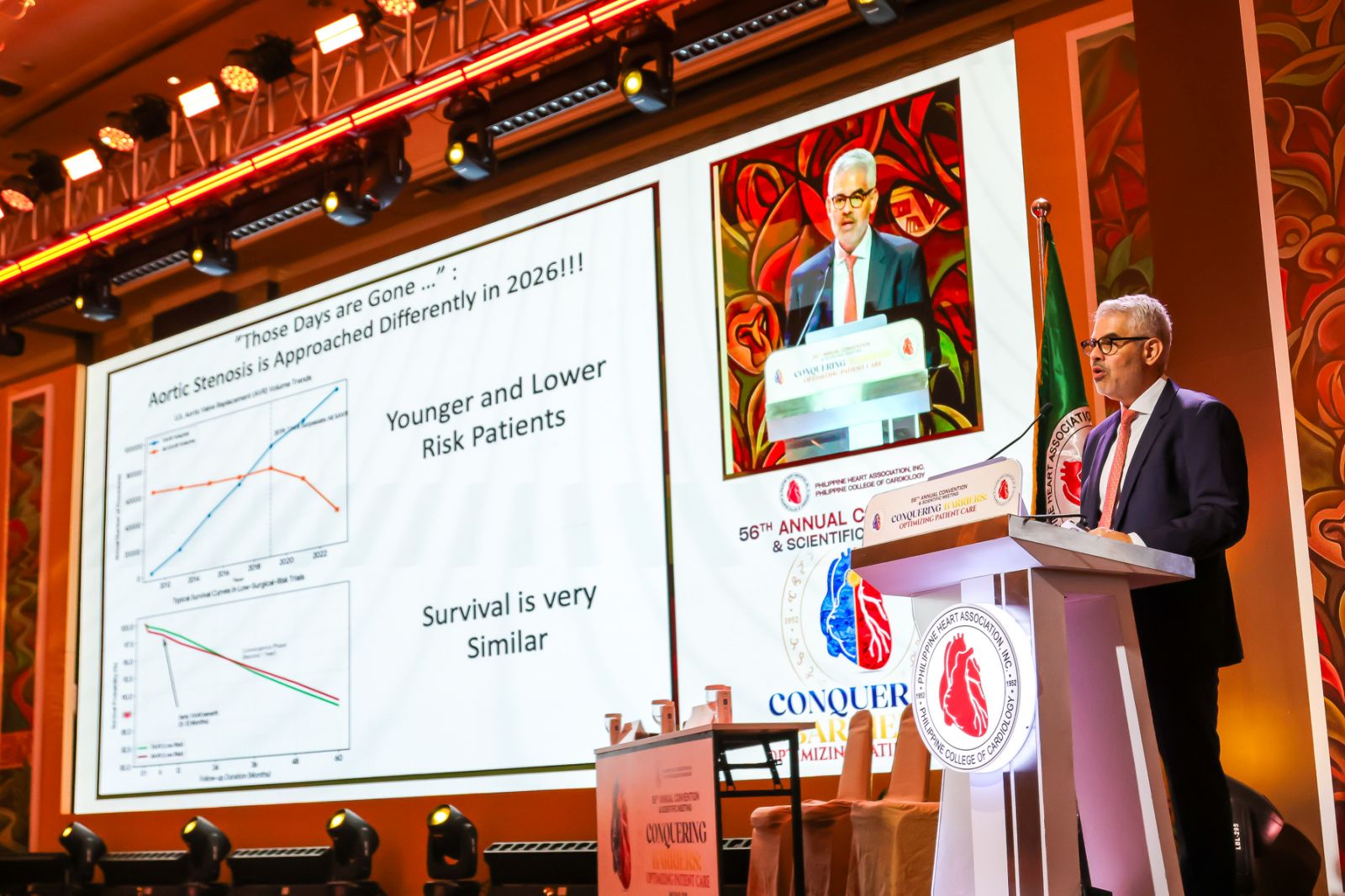
More than a decade later, the landscape has changed dramatically. TAVR is now increasingly performed in younger and lower-risk patients, and in the United States, the number of TAVR procedures has surpassed surgical aortic valve replacement.
That success, however, has created new challenges, said Silva.
For patients in their 60s and 70s who may live for many years after their first valve replacement, the initial procedure may not be their last.
He said physicians must therefore consider not only which treatment is best today, but which strategy will leave the greatest number of options available in the future.
Silva explained that choosing between surgery and TAVR involves much more than age alone. Life expectancy, valve durability, lifestyle considerations, and the likelihood of future procedures must all be part of the discussion.
For many patients, particularly those between 60 and 80 years old, the decision requires an individualized approach rather than a one-size-fits-all solution.
A key part of that planning involves detailed imaging of the heart before any intervention. Physicians must carefully evaluate the anatomy of the aortic root, the position of the coronary arteries, and other structural features that could influence future procedures.
One of the most important considerations is preserving access to the coronary arteries.
As patients age, they may eventually require coronary angiograms or stent procedures. Silva said certain valve designs can make those future interventions more difficult, highlighting the need to think several steps ahead before selecting a valve.
“The valve we plan now does matter,” Silva said.
To illustrate the concept, Silva presented the case of a 69-year-old patient whose anatomy made him a candidate for either surgery or TAVR. Although both options were reasonable, the heart team carefully considered how each choice might affect future treatments.
After discussing the benefits and trade-offs of each approach, the patient ultimately chose TAVR because he wanted to avoid surgery and believed future technology would continue to improve.
The case underscored another major theme of the lecture: shared decision-making.
According to Silva, physicians should guide patients toward the best possible long-term outcomes while recognizing that personal preferences often influence treatment choices.
“The goal is not only to achieve a successful procedure today, but also to preserve future opportunities should additional interventions become necessary,” he said.
As TAVR continues to expand into younger patient populations, Silva encouraged cardiologists to incorporate lifetime planning into routine aortic stenosis management, carefully assess anatomy before intervention, and openly discuss long-term implications with patients.
“The future remains uncertain,” he said, “but the decisions we make today can help ensure our patients are prepared for it.”
