

Introduction
The COVID-19 pandemic has placed an enormous strain on the healthcare systems of the country resulting in a shortage of beds, supplies and medical personnel available for the sick patients flooding the hospitals. This situation might require catheterization laboratories to adjust workflows, practice, procedure and patient prioritization in order to optimize limited resources.
Despite the current focus on COVID related morbidity and mortality, many people still suffer from Acute Coronary Syndrome and other cardiovascular emergencies that will need lifesaving invasive cardiovascular procedures. It is essential that hospitals are still able to provide critical emergency cardiac interventions despite this COVID pandemic.
The risk of COVID 19 infection for the cath lab personnel as well as other patients also need to be urgently addressed. Infection control procedures and adequate personal protective equipment will be discussed in this guide.
For Confirmed/Probable/Suspected COVID-19 patients, (COVID-19 Patients) the benefit that the patient will get from an invasive procedure will have to be balanced with the risk of infection to the staff and other patients as well as to the patients’ risk of dying from the Corona virus infection itself.
This document hopes to serve as a general guide, based on best available evidence and best practices from different institutions, during this present crisis. In all cases, the final decision for each individual patient or institution will be dependent of local expertise, capabilities and resources and the patient’s clinical status.
Depending on the circumstances, a multidisciplinary team approach in COVID-19 patients with ACS including IDS, Pulmonary, Cardiology and Anesthesia services might be helpful.
Patient Selection
Elective patients
In order to avoid overwhelming the limited resources of the hospitals during this pandemic and to reduce the risk of elective patients getting infected in the hospital, it is prudent to defer elective procedures until after the current situation has stabilized. The decision should be individualized to ensure that the patient will suffer no harm due to the delay of his procedure.
STEMI patients
For all patients referred for an intervention, screening for possible COVID-19 infection based on history of exposure, clinical signs and symptoms, as well as an emergency chest X-ray or chest CT Scan when indicated, should be done as soon as possible. A reliable rapid screening test for COVID-19 will be very useful once it becomes available.
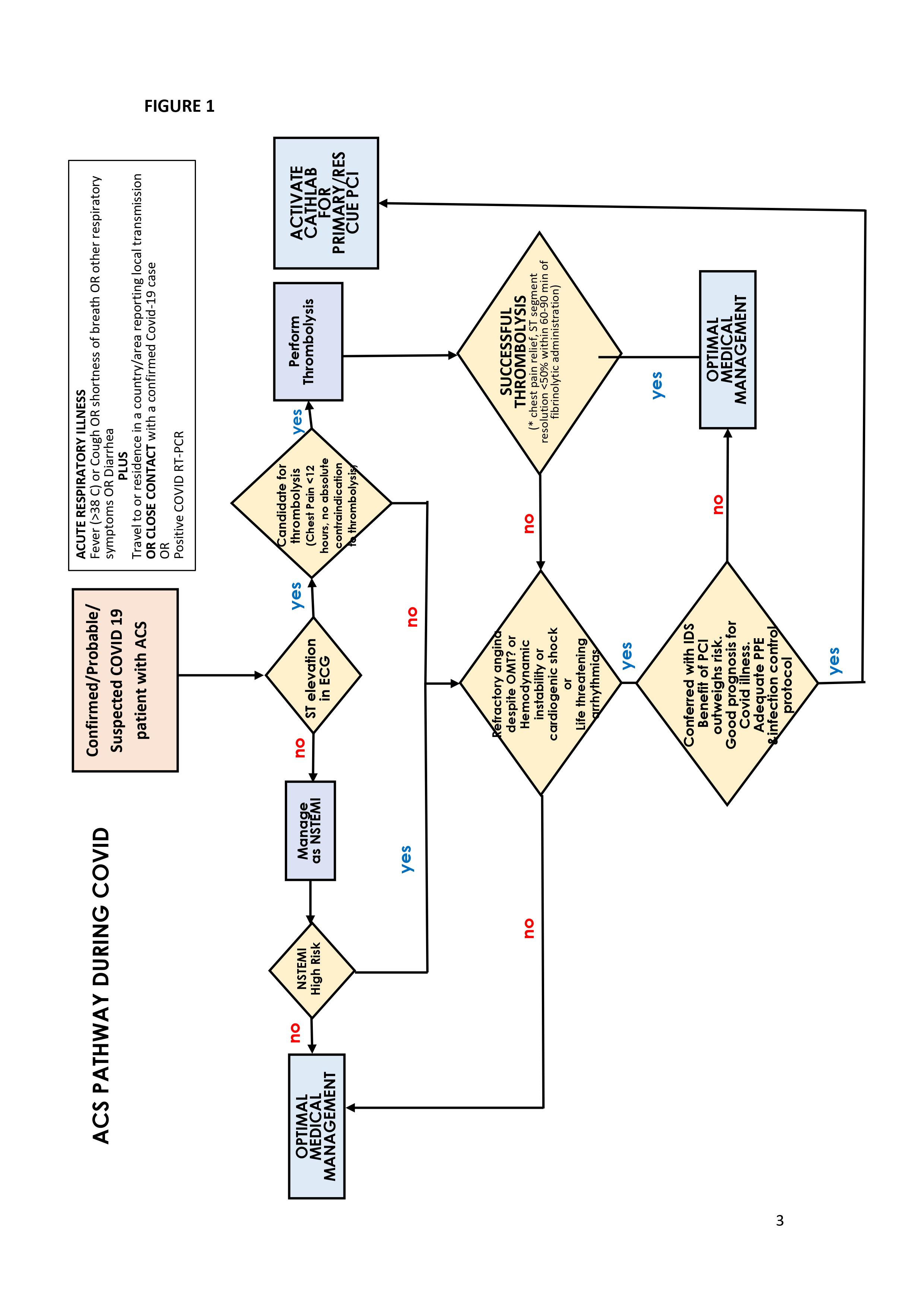
Although most clinical trials show that Primary PCI is the treatment of choice for STEMI, the current limitation in terms of rapid COVID 19 screening, availability of staff, ICU beds, and the risk of possible COVID 19 contamination of the catheterization laboratory may warrant the use of thrombolytic therapy in appropriate patients. Especially for Confirmed/Probable/Suspected COVID-19 patients with STEMI, thrombolytic therapy should be prioritized if they are stable and there are no contraindications. If an invasive treatment strategy is deemed necessary, we have to ensure that the patient will derive significant benefit from the procedure and that there is adequate infection control protocols and personal protective equipment to avoid infection of the cath lab staff and other patients. Below is a proposed algorithm for acute coronary syndrome. (Figure 1)
Non STEMI patients
Risk stratification is highly important for NSTEMI. Screening for COVID-19 infection in these cases should be performed prior to any procedure. For COVID-19 patients, maximal medical therapy is usually sufficient and only patients who are very high risk NSTEMI should be considered for an invasive intervention. In this case, discussion with the infectious disease specialist is recommended to ensure that the patient will benefit from the procedure and that the risk of infection for the staff and other patients can be minimized.
SUCCESSFUL THROMBOLYSIS
Personal Protective Equipment and Infection control in the Cath lab
It is prudent to consider all patients referred for emergency procedures at the cath lab as possible COVID-19 patients and appropriate care should be taken. All patients should wear a mask and all personnel inside the cath lab should wear level 3 or 4 PPE (Scrub suits, N95 mask or better, cap, googles or face shield, double gloves, dedicated footwear/booties, shoe cover, impermeable surgical gown or Hazmat suit (Coveralls). Only the minimum number of personnel should be in the cath lab to reduce the risk of infection and to save on PPE. All staff should undergo training on the proper donning and doffing technique for PPE. (See Appendix A)
Due to the risk of contamination during transport of COVID-19 patients, some procedures normally done in the cath lab (e.g. Central line Insertion, Arterial line, Temporary Pacemaker Insertion) should be done bedside, if possible, using alternative imaging modality like ultrasound.
After each procedure, the appropriate HICU approved disinfection procedure should be performed. Confirmed COVID-19 patients should be done in a dedicated cath lab if possible, if not, these patients should ideally be done last so a terminal disinfection procedure, including UV light disinfection can be performed.
Intubation and CPR in the cath lab
Endotracheal intubation, suctioning and active cardiopulmonary resuscitation are considered aerosol generating procedures and are thought to increase the risk of COVID-19 exposure to personnel. Therefore, COVID-19 patients who require, or will most likely require intubation, should be intubated before the patient is brought to the cath lab. It is also advisable that a specially trained team of anesthesiologist and respiratory therapist handle intubation of COVID-19 patients. Local and international guidelines specifically for COVID-19 patients undergoing CPR are available and can be accessed here (Appendix B). When all reasonable treatment options have been done, DNR option should be considered for COVID-19 patients with guarded or poor prognosis. Nonessential personnel should go out and the cath lab doors should be kept closed during these procedures.
Reference:
- Welt FGP, Shah PB, Aronow HD, Bortnick AE, Henry TD, Sherwood MW, Young MN, Davidson LJ, Kadavath S, Mahmud E, Kirtane AJ, from the American College of Cardiology’s (ACC) Interventional Council and the Society of Cardiovascular Angiography and Intervention (SCAI), Catheterization Laboratory Considerations During the Coronavirus (COVID-19) Pandemic: From ACC’s Interventional Council and
SCAI, Journal of the American College of Cardiology (2020), doi: https://doi.org/10.1016/j.jacc.2020.03.021.
- Unified COVID 19 Algorithms, WHO, PSMID (https://www.psmid.org/unified-covid- 19-algorithms-1/)
- Acute Coronary Syndrome for Covid-19 Related Patients Guideline, St Luke’s Medical
Center
- Catheterization Laboratory Guidelines During COVID19 Pandemic, Philippine Heart Center
- Acute Coronary Syndrome Pathway During COVID Pandemic, UP-PGH Medical Center
- Infection Control Protocol in the Cardiac Catheterization Laboratory, UP-PGH Medical Center
- Philippine Heart Association COVID Resource Center https://www.philheart.org/index.php/education/pha-covid-resource-center
Appendix A: Donning and Doffing of Personal Protective Devices
DONNING: https://drive.google.com/open?id=1eKNo8OwvKP0W6fAQ9edIqsXMuVaFHfnW
DOFFING:
https://drive.google.com/open?id=1NEKgOeSQWpt2Db977S0FM3-rKtNHrcNv
